Blog
My penis is curving!
Underlying condition:
Peyronie’s disease is benign (non-cancerous) build-up of scar tissue in a specific layer of the penis. It can cause your penis to curve, narrow, indent, or hinge. It can lead to weaker erections (less rigid) and may cause pain or shortening. Trauma is the most likely cause. This might be one big injury (penile fracture) or many smaller injuries that build up over years.
What you should know:
Peyronie’s goes through two phases – the acute and the chronic phases. The acute phase can take over a year to complete. Once in the chronic phase, pain associated with Peyronie’s usually goes away, but the curve and changes to your penis typically remain. Peyronie’s rarely gets better without treatment
Treatment options:


The research behind shockwave therapy for ED
Some patients want to really dive into the research behind low-intensity shockwave therapy (Li-SWT) and how it is applied to erectile dysfunction. The recent European Association of Urology (EAU) guidelines on erectile dysfunction provide a nice summary of the current evidence surrounding Li-SWT. The EAU is the first major urologic group to endorse shockwave therapy as a potential treatment for ED patients (the EAU tends to be several years ahead of the American and Canadian Urological Associations).

If you would like to review these guidelines, follow this link:
EAU Guidelines on Sexual and Reproductive Health
If you would like to review the shockwave-specific information, see below:
The use of LI-SWT has been increasingly proposed as a treatment for vasculogenic ED over the last decade, being the only currently marketed treatment that might offer a cure, which is the most desired outcome for most men suffering from ED [418,558-565].
Overall, several single-arm trials have shown a beneficial effect of LI-SWT on patient-reported EF, but data from prospective randomised trials are conflicting, and many questions remain to be answered especially because of the heterogeneity among shockwave generators (i.e., electrohydraulic, electromagnetic, piezoelectric and electropneumatic); type of shockwaves delivered (i.e., focused, linear, semi-focused and unfocused); set-up parameters (e.g., energy flux density and number of pulses per session) and treatment protocols (i.e., duration of treatment, number of sessions per week, total number of shockwave pulses delivered and penile sites of application) [566,567]. In a recent trial trying to assess the best treatment parameters, no significant differences were observed between various energy flux density levels although a 0.10 mJ/mm2 seems to perform slightly better than lower energies [568]. Most of the studies have suggested that LI-SWT can significantly increase IIEF and EHS scores in patients with mild vasculogenic ED, although this improvement appears modest and the rates of patients reporting a satisfactory improvement range between 40-80% [418,566]. A recent RCT reported the proportion of patients with moderate ED attaining a minimal clinically important difference (MCID) in IIEF-EF score significantly improved at three months after treatment (79% in the treatment group vs. 0% in the sham group) [569]. Few studies have shown an improvement in penile haemodynamic parameters after LI-SWT, but the clinical meaning of this improvement remains unclear [566,570]. Likewise, data suggest that LI-SWT could ameliorate erection quality even in patients with severe ED who are either PDE5Is non-responders [563,571,572] or inadequate responders [573], thus reducing the immediate need for more invasive treatments. Treatment effect appears to be clinically evident starting from 1-3 months after treatment completion, with a subsequent progressive decrease of the achieved benefit in terms of EF over time, although some effects could be still detected up to 5 years after treatment [566,568,574]. Data from RCTs suggests that even better results could be achieved by combining LI-SWT with other treatments such as a VED in men with T2DM [575] or daily tadalafil [576]. Combination treatment with LI-SWT and once daily tadalafil led to a 20% higher rate of patients achieving MCID at three months after treatment compared to LI-SWT alone [576].
The impact of LI-SWT has been also tested in the setting of penile rehabilitation after RP. A prospective non-randomised study reported a higher rate of patients reporting an EHS > 3 after LI-SWT and daily tadalafil compared to tadalafil alone six months after surgery [577]. However, two small RCTs showed only a modest advantage for LI-SWT compared to conventional PDE5Is [578,579]. Findings from a recent meta-analysis showed that LI-ESWT showed a significant effect on early recovery of EF in the context of penile rehabilitation of ED after RP. However, the authors clearly outlined that the level of evidence was low; therefore, careful interpretation of the results is required [580].
Overall, larger prospective RCTs and longer-term follow-up data are necessary to provide clinicians with more confidence regarding the use and effectiveness of LI-SWT for ED. Further clarity is also needed in defining treatment protocols that can result in greater clinical benefits [581,582].
As a whole, according to the available data and the novel treatment decision algorithm, the Guideline Panel considers that LI-SWT may be offered to patients with vasculogenic ED, although they should be fully counselled before treatment.
What is erectile dysfunction and how is it treated?
Underlying condition:
Erectile dysfunction (ED) is an issue with the arousal or excitement phase of sexual activity. It is an inability to get and/or keep an erection to satisfy yourself and/or partner.
Risk factors:
Age, smoking, diabetes, high blood pressure, high cholesterol, depression, obesity, sedentary lifestyle.
What you should know:
ED can be a sign of heart disease and other conditions. If you have ED, you should work with your family doctor to treat these issues (e.g. improve blood pressure, cholesterol, blood sugar).
Treatment options:
· Lifestyle modifications – Improve diet, increase physical activity, stop smoking.
· Sexual counselling – Men with ED often benefit from sexual counselling to improve communication with their partner and to overcome performance anxiety.
· Phosphodiesterase type 5 inhibitors (PDE5i) – E.g. sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra). May be combined with testosterone if testosterone levels are proven to be low/borderline low. A common issue that can decrease the effectiveness of these pills is improper use – see the chart at the end of this post.
· Vacuum erection device (VED) – Cumbersome, but a decent low-cost option as you should only need to purchase one: https://www.remingtonmedical.com/product-category/pelvic-health-products/vacuum-erection-pumps/
· Intraurethral suppository (IU) – No needle, but can be painful in its own way. Most patients won’t pursue this option.
· Intracavernosal injection (ICI) – Often involves a combination of alprostadil, papaverine and phentolamine which is self-administered. Not as painful as you would think. Follow this link for an instructional video: https://www.dylanhoaremd.ca/videos/trimix
· Penile prosthesis implantation – Often a last resort, it is a very effective and safe surgical treatment. I typically implant the AMS 700 inflatable penile prosthesis.
· Low-intensity extracorporeal shock wave therapy (ESWT) – Non-invasive, pain free option. Will not work for everyone, but is an excellent option for many men.

Shockwave for erectile dysfunction
Shockwave for erectile dysfunction
Shockwave therapy is a growing option for erectile dysfunction. Originally the idea was rejected by urologists as a sham or ineffective treatment. There is new evidence however pointing towards improved erections in appropriately selected patients. I have had some tremendous success stories.
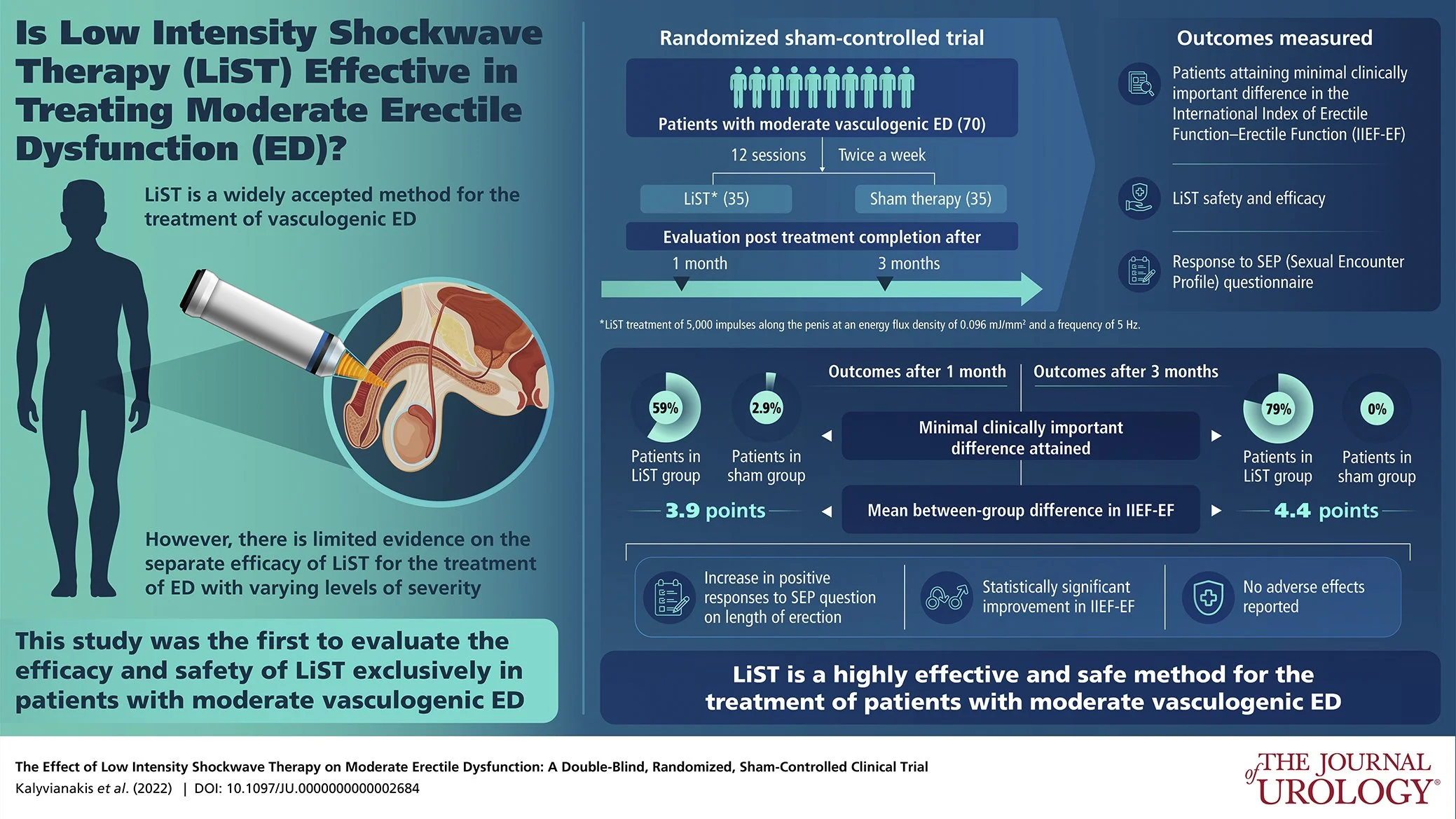
This study by Kalyvianakis et al. was published last year in the Journal of Urology. In my opinion, it is amongst the most thoughtfully designed studies assessing shockwave treatment for erectile dysfunction. It uses a survey called the IIEF to assess improvement in erectile function. It compares patients receiving shockwave therapy (12 treatments, similar protocol to mine) against sham treatment. Patients were assessed at 1 and 3 months after their treatment. The patients receiving shockwave therapy showed improvements in their erections compared to the sham group. Further follow-up is required to know how successful shockwave can be long-term.